
Trends in inequality of opportunity in health over the life cycle: The role of early-life conditions
Kovacic M., Orso C.E., 2022 – Journal of Economic Behavior & Organization
The World Health Organization (WHO) has recently emphasized the importance of reducing health inequalities on a global scale. In the European context, the WHO has promoted the “Health 2020” program with the specific goal of supporting those actions taken by governments to improve the health and well-being of populations, reduce health inequalities, and make access to healthcare systems more efficient and equitable.
Health inequalities can stem from various sources, some of which should not be necessarily evaluated as negative, as suggested by John E. Roemer. He introduced the concept of equality of opportunity, distinguishing between “legitimate” and “illegitimate” sources of inequality. While “legitimate” sources can be attributed to specific individual behaviors, “illegitimate” sources are attributable to circumstances beyond individual choices, such as ethnicity, gender, characteristics of the neighborhood where one grows up, and childhood/adolescent trauma. The impact of these latter circumstances (called “Adverse Childhood Experiences”) on the determination of health inequalities has been little explored so far, although they represent an important factor in the growth and future health of individuals.
In a recent paper entitled “Trends in inequality of opportunity in health over the life cycle: The role of early-life conditions” and published in the Journal of Economic Behavior & Organization, Matija Kovacic and Cristina E. Orso analyze the evolution of inequality of opportunity in the prevalence of chronic disorders over the life course, using an extensive sample of individuals born in different cohorts (from 1940 to 1963) in 13 European countries extracted from SHARE (Survey of Health, Ageing, and Retirement in Europe). Among the chronic diseases considered are heart disorders, respiratory disorders, cancer, diabetes, Parkinson’s and Alzheimer’s diseases, kidney diseases, high blood pressure, high cholesterol, arthritis, osteoporosis, and psychiatric disorders. The authors explore how a set of childhood circumstances (with a special focus on such childhood traumas as physical and emotional abuse by parents, physical violence by third parties, economic and emotional neglect, and the quality of the parent-child relationship) contributes to the determination of these inequalities over the life course.
Figure 1 shows the evolution of the inequality of opportunity in the prevalence of chronic diseases in 13 European countries. The cohorts considered are: 1940-45, 1946-51, 1952-57, and 1958-63. As can be easily seen from Figure 1, inequality of opportunity is not stable over individuals’ lives but tends to be lower at a younger age, and to gradually increase thereafter as individuals age. This trend, which is evident in all the countries considered, albeit with varying intensity, is in line with the “cumulative advantage” hypothesis, according to which adverse events and health disadvantages tend to accumulate as an individual grows older.
Furthermore, inequality of opportunity appears to be more pronounced among individuals belonging to younger cohorts compared to older groups.
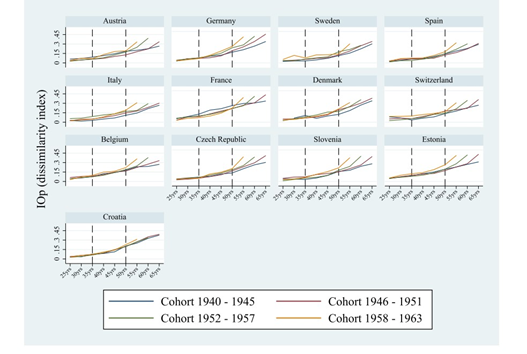
Authors’ analysis based on SHARE data, waves 4-7.
Figure 2 presents the contribution of Adverse Childhood Experiences (ACE) and socioeconomic circumstances (the economic conditions of the family of origin) in shaping the inequality of opportunity at different stages of individuals’ lives (from 25 to 65 years). The most interesting aspect that emerges from the figure is the substantial weight that Adverse Childhood Experiences have in determining these inequalities over the lifespan, comparable in magnitude to that of socio-economic circumstances.
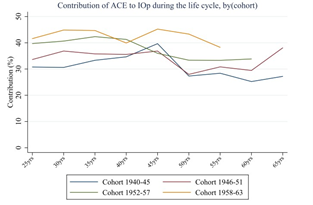
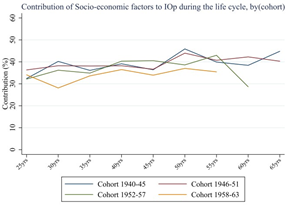
Therefore, traumas experienced during childhood and adolescence play a central and lasting role in determining health inequalities, even in later life, with significant social costs.
In terms of policy implications, it would be desirable to introduce specific programs for the most disadvantaged individuals, such as economic and psychological support for affected families, in order to reduce the “initial” opportunity gap. The recent Covid-19 pandemic has both created new situations of disadvantage, not only in terms of economic costs but also of psychological costs, and exacerbated existing disparities, highlighting the need for timely and targeted interventions to reduce inequalities.